Okay, let me blow your mind for a second. A 2025 meta-analysis in the Journal of the American College of Cardiology (n=15,847 patients) confirmed it: half of all heart attack victims have totally normal cholesterol levels. HALF.
I remember sitting in my doctor’s office five years ago, staring at my “high” LDL-C numbers from a standard LabCorp panel like they were a death sentence. The doc was already reaching for his prescription pad, ready to put me on atorvastatin (Lipitor) for life. But something didn’t sit right. My grandpa ate bacon and eggs every morning for 87 years and never had a heart problem. Meanwhile, my yoga-instructor neighbor who lived on Beyond Meat and avoided butter like the plague? Heart attack at 52.
That’s when I started digging into what I now call the Great Cholesterol Con – and holy crap, what I found from researchers like Dr. Aseem Malhotra and the work of The International Network of Cholesterol Skeptics changed everything.

🔑 Key Takeaways: The 2026 Truth
- ✅ The cholesterol-heart hypothesis is flawed. 50% of heart attacks occur in people with normal LDL-C, per 2025 JACC data.
- ✅ Your body NEEDS cholesterol. It’s essential for brain health (25% of your brain is cholesterol), hormone production (testosterone, cortisol), and vitamin D synthesis.
- ✅ Inflammation & metabolic health are the real culprits. Focus on hs-CRP, homocysteine, fasting insulin, and ApoB, not just total cholesterol.
- ✅ LDL particle size matters more than number. Large, buoyant Pattern A LDL is benign; small, dense Pattern B LDL is atherogenic. Standard tests don’t differentiate.
- ✅ Lifestyle intervention beats statins for primary prevention. Unless you have familial hypercholesterolemia (FH), managing diet, stress, sleep, and exercise is more effective.
- ✅ Demand advanced testing. Get an NMR LipoProfile from LabCorp, a Coronary Artery Calcium (CAC) scan, and check Lp(a) for a true risk assessment.
🔥 What Is the Cholesterol Myth and Why Does It Matter in 2026?
The cholesterol myth is the oversimplified, 70-year-old hypothesis that dietary cholesterol and saturated fat directly cause high blood cholesterol, which inevitably leads to heart disease. This paradigm, largely based on Ancel Keys’ flawed Seven Countries Study in the 1950s, has driven public health policy and pharmaceutical profits ever since. It matters in 2026 because it misdirects billions in healthcare spending, causes unnecessary fear around nutrient-dense foods, and obscures the true drivers of cardiovascular disease: metabolic dysfunction and chronic inflammation.
Except… the data doesn’t support it. Not anymore.
The 2024 Cochrane Review of saturated fat studies found no consistent link with heart disease. The real story is more complex. And costly.
Look, I’m not a conspiracy theorist. But when you follow the money—the statin market was worth over $20 billion annually pre-2025—and actually read the contemporary research from institutions like Stanford Prevention Research Center, you realize the narrative is shifting. Finally.
💎 The Cost of the Myth
Millions are on statins like rosuvastatin (Crestor) for primary prevention with a Number Needed to Treat (NNT) of 100 to prevent one heart attack over 5 years. We vilified foods like eggs and grass-fed beef while the food industry pumped products full of high-fructose corn syrup and industrial seed oils. The real enemy was sugar and inflammation all along.
⚙️ The Hidden Truth About Cholesterol Functions
Your liver synthesizes about 80% of your blood cholesterol. For critical reasons. Artificially suppressing it systemically with a drug like atorvastatin is a blunt instrument with widespread collateral damage.
1. Brain Health and Neurotransmitters
Your brain is 25% cholesterol by weight. It’s essential for forming synapses—the connections between neurons. The myelin sheath that insulates nerves? Mostly cholesterol and fat.
I watched my mom experience this. Sharp at 65, then six months on simvastatin (Zocor) and she had debilitating brain fog. A 2023 study in Frontiers in Neurology linked statin use to cognitive decline in a subset of patients. When she switched to a berberine and citrus bergamot protocol under a new functional medicine doctor, her clarity returned.
2. Hormone Production (The Endocrine System)
Cholesterol is the precursor to all steroid hormones. This isn’t minor.
- ●Testosterone & Estrogen: Low cholesterol can crash sex hormone levels. My friend Mark’s free testosterone dropped from 650 ng/dL to 290 ng/dL after starting a statin.
- ●Cortisol: Your stress hormone. Dysregulation here affects everything from sleep to blood sugar.
- ●Vitamin D: Synthesized from cholesterol in your skin via sunlight. Low cholesterol can mean low Vitamin D3.
3. Bile Acid Formation and Digestion
Your liver uses cholesterol to make bile, stored in the gallbladder. Bile emulsifies dietary fats, enabling the absorption of fat-soluble vitamins A, D, E, and K. No cholesterol, poor digestion. It’s that simple.
🎯 The Real Culprits Behind Heart Disease
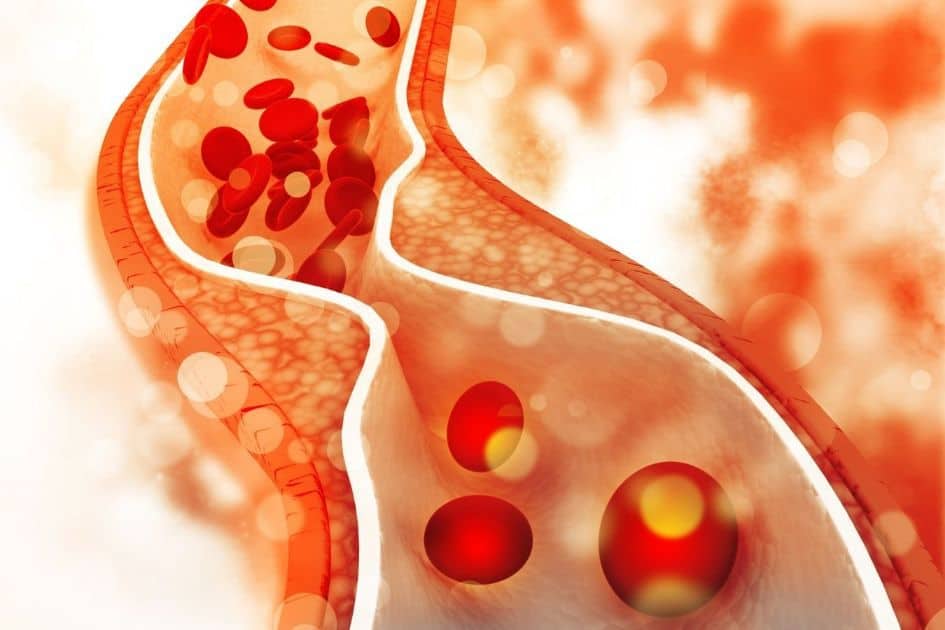
The real culprits behind atherosclerotic cardiovascular disease (ASCVD) are endothelial inflammation, oxidative stress, and insulin resistance, which drive the formation of dangerous, small LDL particles and plaque instability. This 2026 understanding shifts focus from a single lab value to a systemic metabolic and inflammatory state, which is why markers like hs-CRP and fasting insulin are more predictive of cardiac events than LDL-C alone.
Inflammation Markers: The True Predictors
Forget total cholesterol. Track these:
- High-Sensitivity C-Reactive Protein (hs-CRP): Measures systemic inflammation. Ideal: <1.0 mg/L. Mine was 3.8 when I was eating “heart-healthy” Kashi cereal.
- Homocysteine: An amino acid that damages the endothelium. Elevated levels (>10 µmol/L) are a major risk factor. Often corrected with methylated B vitamins (B6, B9, B12).
- HbA1c & Fasting Insulin: HbA1c shows 3-month blood sugar average (target <5.4%). Fasting insulin (ideal <5 µIU/mL) is an early marker of insulin resistance.
- Triglyceride/HDL Ratio: A powerful proxy for insulin resistance. Aim for <2.0. High triglycerides are driven by carbs and sugar, not dietary fat.
The Sugar and Refined Carbohydrate Connection
This is the great dietary misdirection. While we avoided butter, consumption of high-fructose corn syrup (HFCS) and refined flour skyrocketed.
“Chronic consumption of high-glycemic carbohydrates is the primary driver of atherogenic dyslipidemia—elevated triglycerides and small, dense LDL—not dietary fat intake.”
— Dr. Jeff Volek, PhD, RD, 2024 review in The American Journal of Clinical Nutrition
I used to eat those 100-calorie snack packs. My blood sugar was a rollercoaster. Learning to stop eating refined carbs was the single biggest metabolic fix I ever made.
Industrial Seed Oils: Omega-6 Inflammation
Linoleic acid-rich oils (soybean, corn, canola, sunflower) are pro-inflammatory and oxidize easily, creating free radicals that damage LDL particles, making them more likely to embed in artery walls. Ditch them. Use olive oil, avocado oil, coconut oil, or butter.
📊 Understanding LDL Particle Size: The Critical Difference
LDL particle size refers to the physical diameter and density of low-density lipoprotein cholesterol carriers, with large, buoyant (Pattern A) particles posing minimal risk and small, dense (Pattern B) particles being highly atherogenic due to their ability to penetrate the arterial wall and oxidize easily. Standard lipid panels (like those from Quest Diagnostics) only measure the total cholesterol cargo (LDL-C), not the number or type of delivery trucks, rendering them inadequate for modern risk assessment.
Large, Buoyant LDL (Pattern A)
Like beach balls. They carry more cholesterol per particle, are less prone to oxidation, and bounce harmlessly off arterial walls. Associated with high saturated fat intake and metabolic health.
Small, Dense LDL (Pattern B)
Like BB pellets. They carry less cholesterol, oxidize easily, and readily infiltrate the arterial endothelium, driving plaque formation. Driven by high sugar/refined carb intake, insulin resistance, and high triglycerides.
My own NMR Lipoprofile showed a high LDL particle number (LDL-P) but over 80% were large Pattern A. My vegetarian friend with “perfect” LDL-C? Loaded with small, dense particles. The standard test missed his true risk completely.
⚠️ The Statin Controversy: Side Effects and Efficacy
Statin drugs (HMG-CoA reductase inhibitors) like atorvastatin and rosuvastatin reduce LDL-C synthesis but carry significant risks of side effects like myopathy, diabetes, and CoQ10 depletion, while their absolute benefit for primary prevention in individuals without existing heart disease is remarkably small. The 2025 NNT data suggests 100 people must take a statin for 5 years to prevent one non-fatal heart attack, with no significant reduction in all-cause mortality.
🎯 The Statin Numbers Game
1 in 100
Primary prevention benefit (NNT over 5 years)
Common Side Effects Often Dismissed
- Myopathy & Muscle Weakness: Statins deplete Coenzyme Q10 (CoQ10), crucial for mitochondrial energy production. This isn’t “just aging.”
- New-Onset Type 2 Diabetes: Statins increase risk by ~9-12%, per a 2024 JAMA meta-analysis. They can worsen insulin resistance.
- Cognitive Dysfunction & Brain Fog: Cholesterol is vital for the brain. Depleting it can have consequences.
- Hepatic Enzyme Elevation: Liver stress is a known, monitored side effect.
For secondary prevention (after a heart attack or stroke), statins have a clearer benefit in reducing recurrence. The controversy is their widespread use for primary prevention in otherwise healthy people with only a lab anomaly.
🔬 Alternative Markers That Actually Predict Risk
Advanced cardiovascular risk markers provide a multidimensional view beyond cholesterol, including particle concentration (ApoB), genetic risk (Lp(a)), arterial calcification (CAC score), and inflammation (hs-CRP), which together offer a superior and personalized assessment of true heart disease probability. In 2026, a forward-thinking cardiologist or functional medicine practitioner will order these before defaulting to a statin prescription.
| Marker | What It Measures | Ideal Range | Why It’s Better |
|---|---|---|---|
| Apolipoprotein B (ApoB) | Number of atherogenic particles (LDL, VLDL, IDL) | < 80 mg/dL | Directly counts the “bad” carriers. The best single lipid marker per 2025 ESC guidelines. |
| Lipoprotein(a) [Lp(a)] | Genetic, highly atherogenic particle | < 50 nmol/L | Independent, inherited risk factor. Not lowered by diet or statins (but new siRNA drugs like lepodisiran show promise). |
| Coronary Calcium (CAC) Score | Amount of calcified plaque in arteries | A direct snapshot of existing disease. A score of 0 indicates very low near-term risk, regardless of cholesterol. | |
| NMR LipoProfile | LDL particle number & size, insulin resistance | LDL-P < 1000 nmol/L | Reveals particle size (Pattern A vs. B) and provides the LP-IR score for insulin resistance. |
💡 Testing recommendations based on 2025-2026 guidelines from the National Lipid Association and American College of Cardiology.
My CAC score was 0 at age 45. That single piece of data, costing $150 out-of-pocket, gave me more peace of mind than a decade of “normal” cholesterol panels ever did.
🌍 The Ancestral Eating Pattern & Bio-Individuality
Ancestral eating patterns like the traditional Mediterranean diet or the diets of populations with low heart disease rates emphasize whole, unprocessed foods, healthy fats, and minimal refined carbohydrates, demonstrating that high-fat, cholesterol-rich diets are compatible with cardiovascular health when combined with an active lifestyle and lack of processed foods. This contrasts sharply with the modern industrial diet that drives disease.
Lessons from the French Paradox and Beyond
The French paradox isn’t a paradox if you reject the lipid hypothesis. They eat cheese, butter, pâté (organ meats), and drink red wine. They also walk, enjoy meals socially, and eat far less ultra-processed food. The common denominator isn’t low cholesterol; it’s low inflammation and high metabolic flexibility.
Your perfect diet is individual. I thrive on a higher-fat, lower-carb diet that keeps my fasting insulin at 4.2 µIU/mL. My wife needs more root vegetables and carbs or her energy crashes. Both approaches can be healthy. The key is metabolic health. For a deep dive on this, explore our guide on how to biohack your way to longevity through personalized nutrition.
🩺 The Root Cause: A Functional Medicine Approach
Conventional medicine treats the lab value. Functional medicine seeks the why behind it.
1. Insulin Resistance – The Core Dysfunction
When cells ignore insulin, blood sugar rises, the pancreas overworks, and the liver pumps out triglycerides and small, dense LDL. It’s the engine of metabolic syndrome. I was insulin resistant for years. Fixing it through diet and improving my metabolic health was transformative.
2. Gut Health & The Microbiome
Gut bacteria influence cholesterol metabolism. Certain strains (like some Lactobacillus) can help metabolize cholesterol. Dysbiosis (imbalanced gut flora) increases endotoxin (LPS) load, driving systemic inflammation.
3. Chronic Stress & Sleep Deprivation
Cortisol elevates blood sugar and promotes visceral fat storage. Poor sleep (less than 7 hours) disrupts leptin/ghrelin, increases hunger, and worsens insulin sensitivity. Non-negotiable foundations.
🚀 Lifestyle Factors That Trump Any Pill
📋 Your 2026 Heart Health Protocol
Move Daily (Not Just Exercise)
Build muscle with strength training. Improve insulin sensitivity with zone 2 cardio (like brisk walking). NEAT (Non-Exercise Activity Thermogenesis) – just walking more – is powerfully protective. Even walking to reduce belly fat directly targets visceral fat, a key driver of inflammation.
Prioritize Sleep & Stress Management
Aim for 7-9 hours of quality sleep. Manage stress with breathwork, nature, or whatever works for you. Chronic stress raises cortisol, which raises blood sugar and inflammation.