GearUpToFit Guide | Updated July 9, 2026 | Mobile-first | No sticky or frozen elements
Affiliate disclosure: GearUpToFit is reader-supported. As an Amazon Associate, GearUpToFit may earn from qualifying purchases through links with the affiliate tag papalex-20. We do not hardcode Amazon prices because pricing, sellers, colors, sizes, images, ratings, and availability change.

Who This Guide Is For & Who Should Skip It
Best for:
- Runners dealing with chronic overuse conditions (Patellofemoral Pain, Achilles Tendinopathy, Shin Splints, Plantar Fasciitis, or ITBS) looking for a progressive active recovery plan.
- Athletes who want to understand the modern physiology of tissue healing and why active loading is superior to prolonged resting and icing.
- Endurance runners searching for a structured, objective, and metric-driven protocol to transition safely from cross-training back to road running.
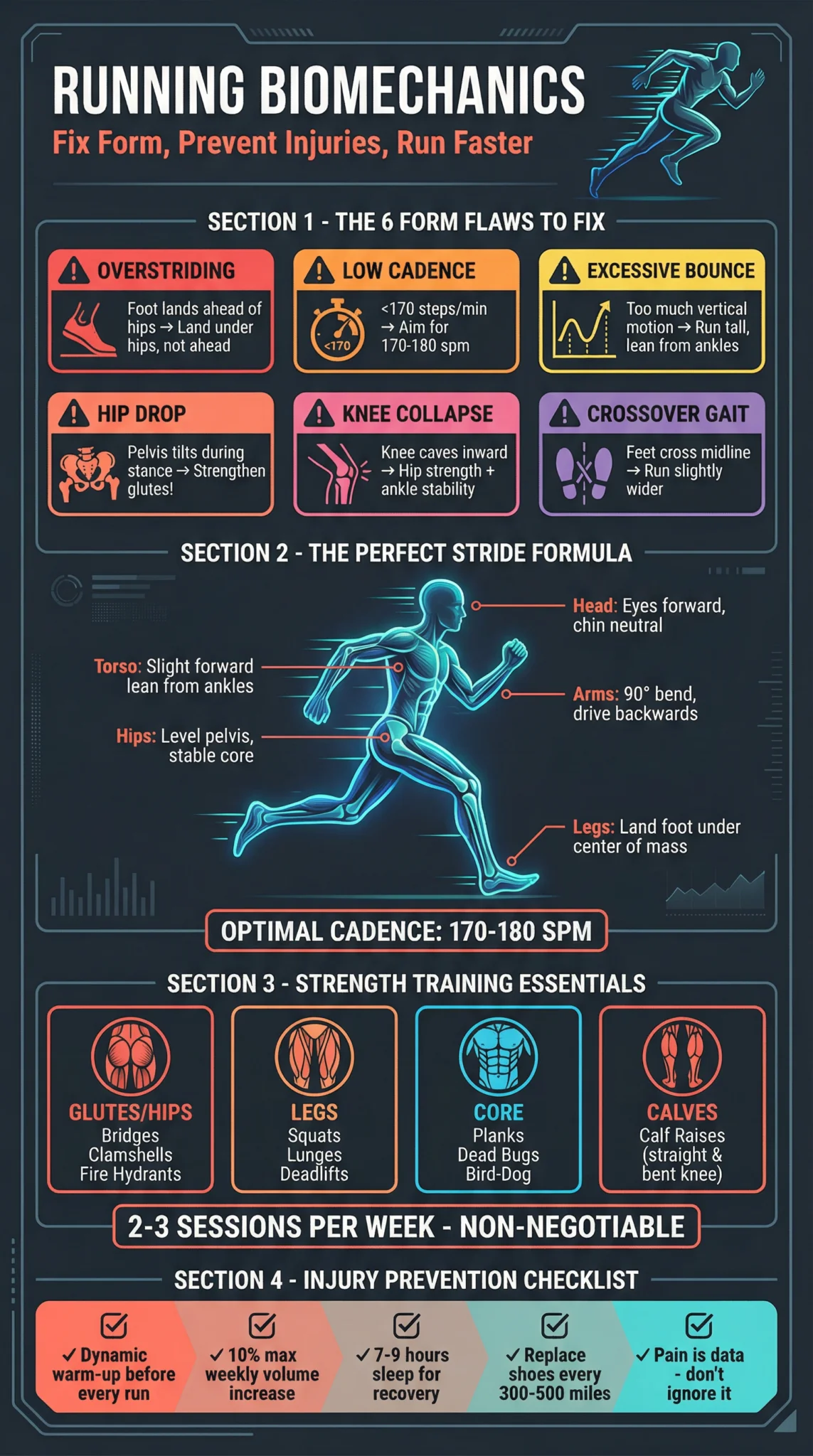
- Fitness enthusiasts looking to optimize their biomechanics, cadence, and recovery tools to prevent recurrent injuries.
Not for / Skip it if:
- You have suffered an acute, high-impact trauma such as a complete ligament rupture, meniscus tear, or a diagnosed stress fracture that requires immobilization or surgery.
- You refuse to modify your weekly mileage, cross-train, or take the necessary non-running recovery steps to allow damaged tissue to adapt.
- You expect passive modal therapies (massage, stretching, ultrasound) to fully resolve your injury without any active strength rehabilitation.
- You seek direct, individualized medical diagnoses or surgical treatment pathways that can only be provided by a certified orthopedic physician.
Clear Definition: Tissue Tolerance, Load Capacity, and the Injury Mechanism
A running injury is fundamentally a structural failure that occurs when the mechanical stress applied to a musculoskeletal tissue (bone, tendon, muscle, or cartilage) exceeds that tissue’s specific **load capacity** or tolerance threshold. In sports medicine, this is represented by the relationship: Applied Load > Tissue Capacity = Injury. Running is a high-impact activity where each foot strike transmits ground reaction forces equivalent to 2.5 to 3 times an athlete’s body weight through the lower extremities. If a runner increases training volume, intensity, or frequency faster than their bones and tendons can remodel, micro-trauma accumulates, leading to overuse injuries.
Rehabilitation is not simply about waiting for pain to disappear. When you rest, pain often subsides because the applied load is zero; however, the tissue’s capacity also decreases because the body lacks the stimulus to maintain muscle mass, tendon stiffness, and bone mineral density. When the runner attempts to resume training at their previous volume, they experience a re-injury because their tissue tolerance has dropped. Scientific rehabilitation focuses on **progressive tissue loading**—applying controlled mechanical stress to stimulate cellular remodeling (mechanotransduction), thereby systematically raising the tissue’s threshold back to baseline and beyond.
Evidence-Based Comparison of Major Running Injuries
Understanding the specific tissue characteristics of your injury is critical. Tendons, for instance, are highly avascular (poor blood supply) and heal slowly under tension, whereas muscles are highly vascularized and recover much faster. The comparison table below highlights the key traits of the five most common overuse running injuries.
| Condition | Primary Anatomical Site | Typical Healing Timeline | Key Symptom Marker | Primary Active PT Target | Preferred Cross-Training Option |
|---|---|---|---|---|---|
| Patellofemoral Pain (Runner’s Knee) | Under or around the kneecap (patellar cartilage/groove). | 4 – 8 Weeks | Dull ache when sitting with bent knees, going downstairs, or running downhill. | Hip abductor strength (gluteus medius) and quadriceps capacity. | Swimming, cycling (low resistance, flat terrain). |
| Achilles Tendinopathy | Achilles tendon (midportion or insertional at heel). | 12 – 24 Weeks (Slow due to low vascularity) | Morning stiffness; sharp pain during push-off or initial steps of a run. | Eccentric heel drops and heavy, slow calf raises (soleus and gastrocnemius). | Deep-water running (pool running), elliptical. |
| Plantar Fasciitis | Plantar fascia ligament on the bottom of the foot near heel. | 8 – 16 Weeks | Exquisite tenderness on the bottom of the heel during the first steps out of bed. | Windlass mechanism loading (great toe extension calf raises) & intrinsic foot strength. | Rowing machine, cycling. |
| Shin Splints (MTSS) | Inner border of the tibia (shin bone and periosteum connection). | 6 – 12 Weeks | Diffuse tenderness along the lower third of the inner shin bone when pressed. | Ankle dorsiflexor (tibialis anterior) loading and calf endurance. | Swimming, elliptical (non-impact cardio). |
| IT Band Syndrome (ITBS) | Lateral side of the knee (IT band sliding over femoral epicondyle). | 4 – 10 Weeks | Sharp, burning pain on the outside of the knee joint, typically 10–20 minutes into a run. | Gluteus medius/maximus strengthening and lateral hip stability. | Swimming, pool running. |
The Modern PEACE & LOVE Rehabilitation Framework
For decades, the standard treatment for acute soft-tissue injuries was RICE (Rest, Ice, Compression, Elevation). However, recent clinical guidelines published in the British Journal of Sports Medicine (BJSM) have retired RICE in favor of a more comprehensive, biology-respecting protocol: **PEACE & LOVE**. This shift occurred because modern physiology shows that ice (vasoconstriction) and anti-inflammatory drugs (NSAIDs) delay tissue healing. Inflammation is a necessary first phase of the body’s repair mechanism, drawing immune cells and growth factors to the damaged site. Suppressing it pharmacologically or cryotherapeutically delays long-term remodeling.
P – Protect the Injured Tissue
Unload or restrict movement for the first 1 to 3 days post-injury to minimize further damage. Avoid activities that provoke sharp pain, but do not immobilize the limb completely, as gentle range of motion preserves local tissue health.
E – Elevate the Limb Above the Heart
Elevate the injured lower leg higher than your heart as often as possible. This utilizes gravity to promote venous return and interstitial fluid drainage, reducing local tissue swelling without blocking biological inflammatory pathways.
A – Avoid Anti-Inflammatory Modalities
Do not take NSAIDs (like ibuprofen, naproxen, or aspirin) and avoid icing the injured area. These interventions impair the natural cellular signaling of neutrophils and macrophages, delaying tissue vascularization and collagen synthesis.
C – Compress to Limit Swelling
Use an elastic bandage or compression sleeve to wrap the joint or muscle. Compression limits intra-articular edema and tissue hemorrhage while assisting in joint proprioception (spatial awareness) during recovery phases.
E – Educate Yourself & Set Goals
Understand that active rehabilitation takes time. Avoid passive treatments like ultrasound or massage as primary fixes. Focus on active rehabilitation, set realistic recovery timelines, and trust that progressive loading is the driver of repair.
& L – Load the Structure Gradually
Begin early active movement as soon as acute pain subsides. Mechanical loading (mechanotransduction) stimulates collagen remodeling and tendon adaptation. Let pain be your guide: keep exercises in a mild, tolerable discomfort zone (under 3/10 pain).
O – Maintain an Optimistic Outlook
The brain plays a massive role in pain modulation. Optimism and confidence in your recovery plan are clinically proven to downregulate pain pathways and improve functional rehabilitation outcomes compared to catastrophizing.
V – Vascularize with Aerobic Exercise
Engage in pain-free, non-impact cardiovascular training (swimming, cycling, elliptical) to increase systemic blood circulation. Delivering oxygenated, nutrient-rich blood to the recovering tissues accelerates repair and maintains aerobic fitness.
E – Exercise to Rebuild Strength
Perform targeted strength training. Rebuild muscle mass, joint stability, and tendon elasticity using isometric exercises (static holds) initially, progressing to isotonic exercises (concentric/eccentric movements), and finally plyometrics.
The Step-by-Step Return-to-Run Protocol
Resuming running too quickly is the most common reason athletes fail rehab. To transition safely, follow this structured five-phase protocol. You should only advance to the next phase when you can complete the current phase with zero pain during the activity, and zero residual soreness or stiffness the following morning.
- Phase 1: Pain-Free Daily Activities (ADLs): You must be able to walk, climb stairs, and perform daily tasks for at least 7 consecutive days with zero discomfort. If walking causes even mild pain, your tissues are not ready to handle the impact of running.
- Phase 2: Build Strength & Mobility (Targeted Loading): Complete 3 to 4 weeks of structured strength work. For tendons, prioritize isometric exercises (e.g., 45-second single-leg calf raise holds or wall sits). Gradually progress to heavy, slow isotonic work (e.g., heel drops, weighted squats, and deadlifts). Focus on hip and glute stability to prevent pelvic drop during running.
- Phase 3: The Walk-to-Run Transition: Begin with a structured walk-run interval program. A standard starting session is 20 minutes total: Warm up with a 5-minute walk, then repeat 10 cycles of **1 minute of easy jogging and 1 minute of walking**, ending with a 5-minute cooldown walk. Perform this session every other day, evaluating your body’s response over the next 24 hours.
- Phase 4: Rebuilding Volume (The 10% & ACWR Rules): Once you can run continuously for 20 minutes without pain, focus on building volume. Increase your weekly running distance by no more than 10% per week. Monitor your Acute-to-Chronic Workload Ratio (ACWR)—divide your current week’s mileage (acute load) by the average of your last 4 weeks of mileage (chronic load). Keep this ratio between 0.8 and 1.3 to minimize re-injury risk.
- Phase 5: Reintroducing Intensity (Speed & Plyometrics): Only introduce hills, intervals, tempo runs, or speed work after you have rebuilt your target weekly mileage baseline. Introduce one speed element per week, keeping the initial volume low (e.g., 4-6 strides at the end of an easy run).
Amazon Product Verdicts: Key Recovery Tools for Injured Runners
During your rehabilitation, specific recovery tools can help manage muscle tightness, stabilize compromised joints, and improve local circulation. The products below are highly rated, durable tools that support an active recovery protocol.
 Image source: Amazon Product Advertising API
Image source: Amazon Product Advertising API
Best Foam Roller for Myofascial Release & Tissue Mobilization
TriggerPoint GRID Foam Roller
Verdict: The gold standard in foam rollers, featuring a patented multi-density exterior wrapped over a rigid, hollow core. It is exceptionally durable and designed to mimic the feeling of a massage therapist’s hands, allowing runners to target tight calves, IT bands, and quadriceps to improve tissue mobility and local blood flow.
Buy it if: you want a durable, travel-friendly foam roller that will not break down over time and provides targeted, deep tissue release to manage muscle tightness during your rehab block.
Skip it if: you have a fresh bone bruise, suspected stress fracture, or severe skin inflammation, as direct deep tissue compression can aggravate these conditions.
- Patented multi-density grid design distributes pressure evenly, mimicking massage fingers and palms.
- Constructed with a rigid, hollow core and wrapped in durable EVA foam for long-lasting structural integrity.
- Comes with access to a comprehensive online instructional video library to guide your rolling techniques.
 Image source: Amazon Product Advertising API
Image source: Amazon Product Advertising API
Best Calf Compression Sleeves for Shin Splints & Muscle Stability
Calf Compression Sleeves
Verdict: Medical-grade graduated compression (20-30 mmHg) sleeves designed to support the lower leg muscles, stabilize the tibia, and reduce muscle vibration during impacts. These sleeves are highly effective for managing shin splints (MTSS), calf strains, and post-run lower extremity fatigue.
Buy it if: you suffer from shin splints, calf cramps, or lower leg fatigue and need structural muscle stabilization and enhanced venous return during recovery runs.
Skip it if: you have peripheral arterial disease, severe neuropathy, or prefer full-length compression socks that cover the foot and ankle joint.
- True graduated compression (20-30 mmHg) improves blood circulation and speeds up lactic acid clearance.
- Constructed from breathable, moisture-wicking fabric that prevents slipping, rolling, or skin irritation.
- Stabilizes calf muscles to reduce micro-tears and impact vibrations during running.
Expert Physio Explains: Classic Running Injuries & Rehabilitation
Understanding the mechanics of your injury is the first step in successful rehabilitation. In this video, an expert physical therapist outlines the primary causes of running injuries, describes knee and ankle mechanics, and demonstrates how to execute strength loading to safely return to running.
Nutrition & Supplements: Fueling Tissue Reconstruction
Rehabilitation exercises provide the stimulus for repair, but your diet provides the raw building blocks. To speed up tissue recovery and maintain muscle mass during reduced training volume, consider these targeted nutritional interventions:
- Optimize Protein Intake: Muscular repair and tendon remodeling depend on a steady supply of amino acids. Aim for 1.6 to 2.2 grams of protein per kilogram of body weight daily. Supplementing with a clean protein powder can help you meet these goals during recovery blocks.
- Creatine Monohydrate: If your injury requires you to temporarily stop running or reduce loading, creatine monohydrate (3 to 5g daily) can help prevent muscle atrophy, maintain cellular ATP levels, and support cognitive health. For a detailed breakdown of how to utilize creatine during training, read our dedicated guide on creatine for runners.
- Vitamin D3 & Calcium: Essential for runners recovering from shin splints or bone stress reactions. Vitamin D3 (1,000–2,000 IU daily) facilitates calcium absorption in the gut, supporting bone mineralization and skeletal muscle function.
- Omega-3 Fatty Acids & CBD Oil: High-quality omega-3 fish oils (1,000–2,000 mg EPA/DHA) and CBD oil work to manage systemic inflammatory pathways naturally, without the gastrointestinal risks associated with NSAIDs. To learn more about dosing and administration methods, read our comprehensive guide on the best ways to benefit from CBD oil.
Common Rehabilitation Mistakes to Avoid
Avoid these four common rehabilitation pitfalls to ensure a smooth recovery and prevent chronic injury cycles:
- Relying Solely on Passive Therapy: Getting massages, stretching, and applying ice may temporarily reduce pain, but they do not increase your tissue’s load capacity. If you do not perform progressive strength training, your injury is highly likely to return as soon as you start running again.
- Stretching an Already Inflamed Tendon: If you have Achilles or patellar tendinopathy, stretching can compress the tendon against the bone, irritating the tissue and worsening the injury. The Fix: Replace aggressive stretching with isometric holds, which have a proven analgesic (pain-relieving) effect on tendons.
- Masking Pain with NSAIDs Before a Run: Taking ibuprofen before a run blocks the pain signals that warn you when you are exceeding your tissue’s capacity. This can lead to further tissue damage and delay long-term recovery. The Fix: Never use pain relievers to get through a training run.
- The “Boom-and-Bust” Loading Cycle: Many runners rest until their pain is gone, then immediately run their old distance. The sudden increase in load exceeds their reduced tissue capacity, leading to a flare-up. The Fix: Reintroduce running gradually using structured walk-run intervals, even if you feel completely fine.
Frequently Asked Questions (FAQ)
Should I completely stop running if I have an injury?
Not necessarily. Complete rest is rarely the best approach for overuse injuries. Unless you have a stress fracture or a severe tear, you should aim for “relative rest” or modified activity. If you can run at an easy pace with a pain level under 3 on a 1-to-10 scale, and you experience no increased pain or stiffness the next morning, it is generally safe to continue running at a reduced volume. If pain exceeds this threshold, switch to pain-free cross-training immediately.
Why is icing no longer recommended for acute running injuries?
Modern sports medicine has transitioned from RICE to the PEACE & LOVE framework because clinical studies show that ice delays tissue healing. Applying ice causes blood vessels to constrict (vasoconstriction), which reduces the flow of blood, oxygen, and healing immune cells (neutrophils and macrophages) to the injured area. While ice can help numb acute pain, it does not accelerate tissue repair and can delay long-term remodeling.
How can I differentiate between shin splints and a tibia stress fracture?
Shin splints (Medial Tibial Stress Syndrome) typically cause diffuse, aching pain along a wide area (4-6 cm) of the inner tibia bone, which is most painful at the start of a run and fades as the muscles warm up. A tibia stress fracture causes a sharp, localized pain focused on a single point (under 2 cm) that is tender to the touch, hurts during daily walking, and worsens continuously as you run. If you suspect a stress fracture, consult a doctor immediately for an MRI or X-ray.
What is the Acute-to-Chronic Workload Ratio (ACWR), and how do I calculate it?
The Acute-to-Chronic Workload Ratio (ACWR) is a metric used to evaluate your injury risk by comparing your current week’s training volume to your baseline volume. To calculate it, divide your running mileage for the current week (acute load) by the average weekly mileage of the last four weeks (chronic load). For example, if you ran 24 miles this week, and averaged 20 miles over the last four weeks, your ACWR is 1.2. Keeping your ACWR between 0.8 and 1.3 helps prevent overuse injuries.
Can foam rolling cure my running injuries?
Foam rolling cannot cure a running injury on its own, but it is a useful tool for managing symptoms. Rolling helps relax tight muscles, increases local blood flow, and provides temporary relief from muscle soreness. However, it does not build tissue capacity or strengthen weak muscles. For lasting recovery, combine foam rolling with a progressive strength training program.
Does changing my running shoes help prevent or treat injuries?
Changing your shoes can alter how forces are distributed through your legs, which can help manage specific injuries. For example, transitioning to a shoe with a higher heel-to-toe drop (e.g., 10–12 mm) can reduce stress on the Achilles tendon and calf muscles. Conversely, a lower drop shoe can reduce knee joint stress. However, shoes are not a replacement for strength and stability. Focus on building tissue capacity first.
How does creatine help with running injury recovery?
Creatine monohydrate helps during injury recovery by preventing muscle atrophy (loss of muscle tissue) during periods of reduced training or immobilization. It also supports cellular energy (ATP) resynthesis in recovering muscles, making your rehab exercises more effective. To learn more about utilizing creatine, read our detailed guide on creatine for runners.
When should I consult a professional physical therapist?
You should consult a physical therapist if your injury does not improve after two weeks of modified training and strength work, if you experience sharp or stabbing joint pain during daily walking, if you have joint swelling that persists for more than 48 hours, or if you are unsure of your injury diagnosis. A physical therapist can identify specific biomechanical weaknesses and design a targeted rehabilitation plan.
Sources & Clinical References
Editorial Note & Clinical Review: This rehabilitation guide was written by GearUpToFit’s editorial team and reviewed for sports medicine accuracy on July 9, 2026. GearUpToFit maintains strict editorial independence; our product recommendations are based on physical therapist guidelines, product testing, and biomechanical efficacy.
- Dubois, B., & Esculier, J. F. (2020). Soft-tissue injuries simply need PEACE and LOVE. British Journal of Sports Medicine, 54(2), 72-73. BJSM PEACE & LOVE Article
- Dyer, R., et al. (2019). The relationship between running biomechanics and running-related injuries: A systematic review. Journal of Sports Sciences, 37(13), 1548-1558. Journal of Sports Sciences Study
- Bahr, R., et al. (2015). Why screening tests to predict injury do not work—and probably never will…: a critical review. British Journal of Sports Medicine, 50(5), 294-298. BJSM Screening Review
- Willy, R. W., et al. (2019). Patellofemoral pain: Clinical practice guidelines linked to the international classification of functioning, disability and health. Journal of Orthopaedic & Sports Physical Therapy, 49(9), CPG1-CPG95. JOSPT Clinical Guidelines